

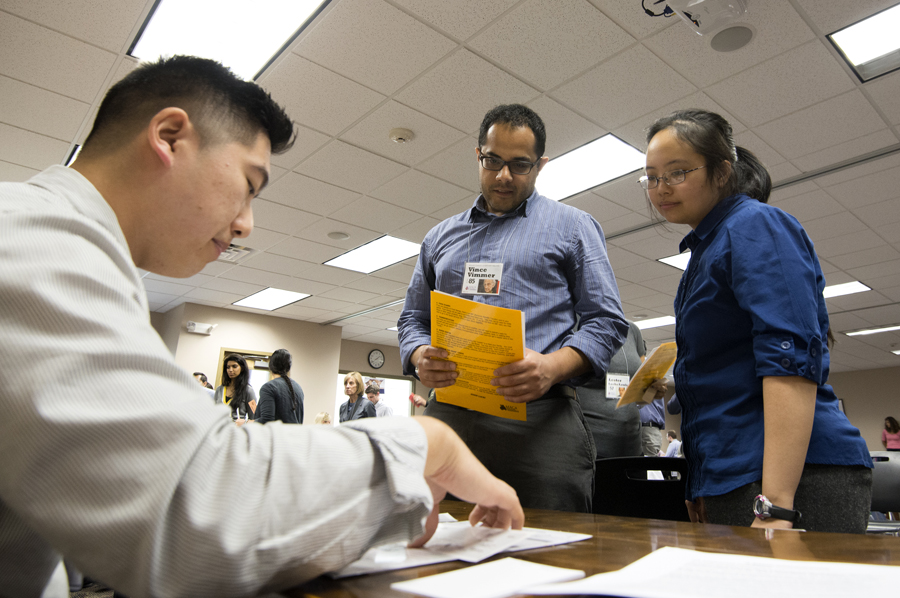
Pharmacy student Johnny Wang (behind desk) plays a banker serving low-income clients portrayed by residents Ramtin Samie, MD, and Winnie Tsao, MD.
Simulation Helps UB Medical Trainees Understand Poor Patients
Published August 25, 2014 This content is archived.
Story by Suzanne Kashuba
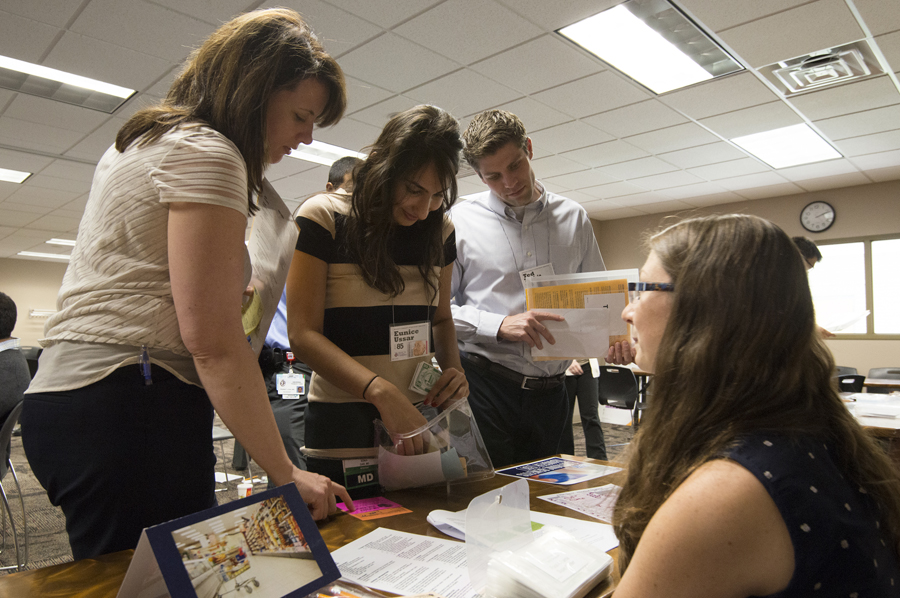
For one eye-opening afternoon, University at Buffalo resident physicians and medical students got a small taste of the challenges and frustrations patients living in poverty or on a low income face every day.
Forty family medicine residents and 15 medical students engaged in a simulation exercise designed to give them a realistic idea of what it takes to make ends meet when financial resources are scarce.
Pretending to Be Poor: Transforming Personas
Participants took on new identities as they personified written scenarios describing their new names, life circumstances and available resources.
Their new persona may have just lost a job or been deserted by the family breadwinner. They may be homeless or receiving public assistance. They may be a senior citizen on Social Security, or a grandparent raising grandchildren.
Despite diverse roles, the personas all had the same challenge: to provide basic necessities for themselves and their families throughout a simulated month — four 15-minute “weeks.”
The “families” are both helped and hindered by various community service providers, portrayed by volunteers, including UB faculty and staff members. The providers include, for example, a police officer, pawnbroker, grocer, landlord, a payday lender, social service worker, employer, child care worker and teacher as well as an “illicit activities person,” who may sell drugs or steal.
As the personas moved around the volunteer-staffed tables representing services, they tried their best to navigate the obstacles of daily existence — but found it wasn’t easy.
As volunteer Pam Coniglio, clerkship coordinator for family medicine, observed, “the residents really were stressed, frustrated and angered by the system and their inability to easily get the things they needed to maintain their households and their jobs.”
The experience “reinforced the need for everyone to take a step back before making assumptions,” said volunteer Karen Devlin, family medicine program coordinator for predoctoral education. “You need to walk a mile in someone’s shoes before forming an opinion.”
‘Broadening Horizons’ About Patient Experiences
Kim Griswold, MD, MPH, associate professor of family medicine and psychiatry, described the experience as “fantastic.”
“There were real interactions,” said Griswold, who served as a volunteer and also led a debriefing session for participants focused on implications for patient care.
This experience “broadens horizons about what patients experience,” she said. It helps participants understand the numerous barriers their patients may face, including financial and time constraints, transportation needs and language difficulties.
One participant was forced to “visit” the Department of Social Services three times before he met with his caseworker because he kept arriving as the office was about to close.
As first-year resident Karim Velji said shortly after completing the exercise, “I think I began to appreciate the truths of what my patients might experience and felt myself even just today be more considerate and empathetic toward them.”
Paradoxically, although one of the simulation tables represented a medical station, the exercise suggests that people in poverty may forgo needed health care. “Only one person went to the clinic,” Griswold noted. “People didn’t have time to go to the doctor. They need us, but can’t get there.”
“I have been clueless to many struggles that my inner-city patients and families face,” admitted Daniel W. Sheehan, MD, PhD, clinical associate professor of pediatrics and chief of pediatric pulmonology, who volunteered at the event. In the future, he said, he will “take the time to delve into social barriers to adherence and self-care.”
Understanding Needs in the Buffalo Area
“The exercise also helps participants understand urban medicine in particular and opens their eyes to the poverty rate and low income levels in Buffalo,” Griswold says.
Buffalo typically ranks among the poorest large cities in the nation. Based on recent U.S. Census Bureau data, it is the fourth poorest city for families, with 26.4 percent of families living below the federal poverty level. Median household income amounted to slightly more than $30,500 per year from 2008 to 2012.
Although third-year medical students have been participating in the poverty simulation exercise for a few years, this is the first time it has been offered to UB medical residents.
UB’s Office of Graduate Medical Education and Department of Family Medicine residency program collaborated with the United Way of Buffalo and Erie County to conduct the training experience.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Grand Rounds
No events scheduled.